
Podcast: Play in new window | Download
Subscribe: RSS
[display_podcast]
Date: January 28, 2014
Guest Skeptic: Dr. Philippe Rola who graduated from McGill University in Internal Medicine. He is chief of ICU at Santa Cabrini Hospital in Montreal and an attending ICU specialist at Scarborough General Hospital in Toronto. Co-founder and president, critical care and ultrasound institute (www.ccusinstitute.org). A social media newbie (www.thinkingcriticalcare.com @ThinkingCC).
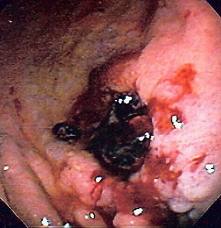
Dr. Rola came to my attention because of the great blog post he wrote on the paper we are reviewing today. It was called “But doctor, he’s vomiting blood!!!”.
Case Scenario: A 62-year-old man arrives with hematemesis. BP 112/72, HR 84 and Hgb is 82 (8.2g/dl).
Question: Which is better, a conservative or liberal transfusion strategy for upper GI bleeds?
Background:
- Common ED presentation
- High morbidity and mortality
- Transfusions can be lifesaving in massive bleed
- Controversy for less serious cases
- Observational studies of small controlled trials suggest transfusions may be harmful in patients with hypovolemia anemia
- Animal studies suggest harmful if bleeding from portal hypertensive source due to rebound increased in portal pressure which is associated with a risk of re-bleeding.
- PC Hebert et al. A Multicenter, Randomized, Controlled Clinical Trial of Transfusion Requirements in Critical Care (TRICC). NEJM 1999; 340:409-417February 11, 1999DOI: 10.1056/NEJM199902113400601
Reference: Villanueva et al. Transfusion Strategies for Acute Upper Gastrointestinal Bleeding. NEJM 2013;368:11-21. DOI: 10.1056/NEJMoa1211801
- Population: Adults (n=921) with upper GI bleeds
- Intervention: Restrictive strategy (<7g/dl) or Liberal (<9g/dl)
- Control: None
- Outcome: Death at 45 days, re-bleeding and adverse outcomes
- Inclusion:
- 18 years and older
- hematemesis/blood in NG, melina or both
- Excluded
- Declined blood transfusion
- Massive bleed
- ACS, TIA or CVA
- Recent transfusion (90d), trauma or surgery
- Lower GI bleeds
- Previous decision by physician that patients should avoid specific medical therapy, Rockall Score of 0 with HgB >12g/dl
- Inclusion:
Rockall Score: This is a scoring system that attempts to identify patients at risk of adverse outcome following acute upper gastrointestinal bleeding. Rockall et al. identified independent risk factors in 1996 which were later shown to predict mortality accurately. The scoring system uses clinical criteria (increasing age, co-morbidity, shock) as well as endoscopic finding (diagnosis, stigmata of acute bleeding). A convenient mnemonic is ABCDE – i.e. Age, Blood pressure fall (shock), Co-morbidity, Diagnosis and Evidence of bleeding.

Authors’ Conclusions: “As compared with a liberal transfusion strategy, a restrictive strategy significantly improved outcomes in patients with acute upper gastrointestinal bleeding.”
 Randomized Clinical Trial Quality Check:
Randomized Clinical Trial Quality Check:
- ED patients – Unsure (did not get randomized into the study until after admission)
- Randomized – Yes
- Concealed – Yes
- Analyzed – Yes
- Consecutive – Unsure
- Prognostic Factors – Yes
- Unaware Allocation – NO
- Treated Equal – NO (PUD patients got PPI bolus plus drip for 72hrs [NEWMAN], portal HTN patients received IV somatastatin and prophylactic antibiotics, bleeding esophageal varicies were treated with bands or sclerotherapy, and non-bleeding varices were injected with cyanoacrylate)
- Follow-up – Yes
- Patient Oriented Outcome – Yes
- Large and Precise – Yes
Results:
- Mortality at 45 days:
- 5% (23 patients) vs. 9% (41 patients)
- HR=0.55; (95% CI 0.33-0.92)
- NNT=25
- Further Bleeding:
- 10% (45 patients) vs. 16% (71 patients)
- HR=0.68 (95% CI 0.47-0.98)
- NNT=17
- Overall Adverse Events:
- 40% (179 patients) vs. 48% (214 patients)
- NNT=13

BEEM Commentary: This was a good study asking a very important question, when to start transfusion in acute upper GI bleeds. They generated their hypothesis based on a number of considerations. These included trials in critically ill patients (TRICC NEJM 1999), observational studies, small RCTs and animal studies.
While the patients were randomized there was a possibility of selection bias based on the exclusion criteria of the Rockwell Score. They did not include patients at low risk of bleeding and those with massive bleeding. Massive bleeding was not adequately defined in the manuscript. There was no control group in the study design. This introduces bias because patients and physicians were not blinded to allocation. They state it is unlikely any bias would effect their primary outcome of death at 45 days. This seems suspect for a couple of reasons. There were 39 patients (9%) major protocol violators in the restrictive strategy vs. only 15 (3%) in the liberal group. Each group received one unit of blood up front. Then it was at the discretion of the attending physicians when subjective symptoms of anemia developed, massive bleeding occurred or when surgical intervention was required. This may have greater impact than the authors suggest.
- NNT for Death at 45 days = 25 (95% CI 13.5-154.7)
- NNT for Re-Bleed = 17 (95% CI 9.8-71.0)
- NNT prevent Adverse Event = 13 (95% CI 7.0-79.0)
Another important consideration was all patients got endoscopy within the first 6 hours. This may not be what happens at your primary place of practice.
This study seems to be consistent with the other smaller studies, observational studies, animal studies and those critically ill patients without acute upper GI bleeds. Most of this protocol takes place outside the emergency department. However, the first unit of blood often gets started in the emergency department. This would suggest that being more conservative than liberal has more benefit and less harm in these patients.
The Bottom Line: When it comes to transfusion strategies for acute upper GI bleeds, less may be more.
Case Resolution: You group and cross him for 2 units of blood, hang one unit of blood in the emergency department, give pantoprazole 40mg IV and consult GI service.

Clinical Application: I will probably be less likely to provide blood to patients with non-massive, acute upper GI bleeds with initial hemaglobins of >7g/dl.
What do I tell my patients? Sometimes giving blood can cause harm and not be helpful. We are going to see what your hemoglobin before starting a transfusion. If it is really low you will need some blood but if it is not too low we will discuss the case with the admitting specialist to make sure we are giving you the best care.
How is this going to change your practice once this patient arrives in the ICU?
KEENER KONTEST: Last weeks winner was Justin Losier from the University of Ottawa. He knew that Allen Ginsberg wrote the poem Howl.
Listen to the SGEM podcast to hear the keener question. If you know the answer send an email to TheSGEM@gmail.com with Keener Kontest in the subject line. The first person with the correct answer will win a cool skeptical prize.
BEEM Conferences: SteelBEEM, SweetBEEM and PrairieBEEM




{kind=link}
You must be logged in to post a comment.