
Podcast: Play in new window | Download
Subscribe: RSS

Buckle Fracture
Fractures of the distal radius are the most common fractures in childhood (Landin et al). There is a difference between buckle fracture and greenstick fractures.
Buckle fractures (also called torus) are defined as a compression of the bony cortex on one side with the opposite cortex remains intact. In contrast, a greenstick fracture the opposite cortex is not intact.

Greenstick Fracutre
There seems to be a variety of approaches to the treatment of buckle fractures(cast vs. splint and lenght of immobilization). A survey done over a decade ago in Canada demonstrated this variablity (Plint et al 2003). There is even an apparent devide between North America (favour casting) (Plint et al 2004) vs. Europe (favour splinting) (Plint et al 2006).
Question: Cast vs. splint for buckle fracture and appropriate follow-up?
As with most evidence based medicine (EBM) it can be a little messy. As my mentor, Dr. Andrew Worster from McMaster always says…the EBM answer is always “it all depends”.
Looking back through the literature without commenting on every single article on the subject here are some highlights. I want to mention these before the critical review of two more recent articles on the subject.
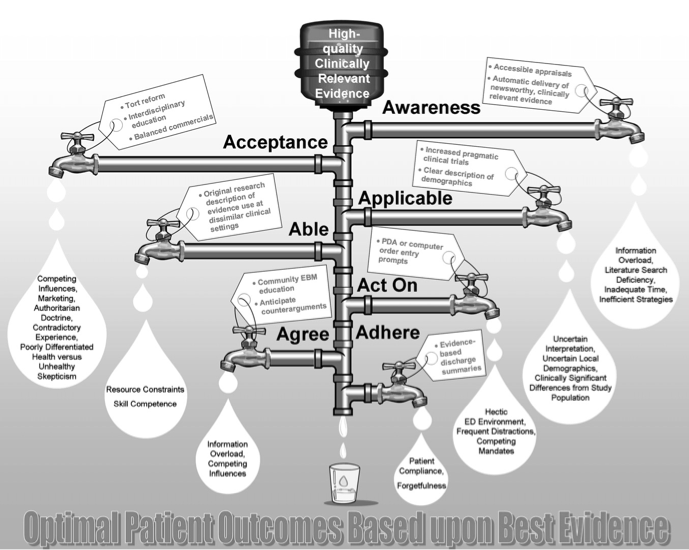
Why discuss such old data from nine years ago? As SGEM listeners know it takes an average of ten years for high quality, clinically relevant inforamtion to reach the patients bedside. This case was an excellent opportunity to address this knowledge translation problem.
The father of the patient told me the doctor at the peds emerg said splinting would be OK but they were going to put a full cast on anyways. This is one of the key leaks in the Pathman pipeway. The academic centre was AWARE of the evidence but did they ACCEPT, AGREE, able to ACT upon or ADHERE to the evidence?
Plint et al (2004) mentioned earlier published a retrospective chart review of 309 children with buckle fractures of the distal radius or ulna. The average age was 9 years old. They found no benefit to casting vs. splinting.
- None needed a reduction
- None needed orthopedic intervention
- No displacement of their fracture
Potential harm:
-
- Orthopedic visits (time for parents and child)
- Repeat xray
- 12% in casted group had subsequent ED visit for cast problems
There are limitations to a retrospective study being conducted at a single site. In addition, 11% of patient were lost to follow-up. With these limitations the authors concluded “Orthopedic follow-up visits and radiographic follow-up may have minimal utility in the treatment of pediatric wrist buckle fractures. ED casting may pose more risk than benefit for these children. Splinting in the ED with primary care follow-up appears to be a reasonable management strategy for these fractures. A prospective study comparing ED splinting and casting for pediatric wrist buckle fractures is needed”.
Plint et al rose to the challenge of a prospective trial in 2006. They published a RCT of removable splinting vs. casting for wrist buckle fractures in children. This study had n=87 with average age 9 years old. They used a self-reported outcome tool called Activities Scales for Kids performance version (ASKp). The main outcome was the ASKp score at 14d post injury which favoured splinting over casting.
Results:
- No difference in pain
- Better function with splint
- Less difficulty with daily activities (ex. bathing/showering)
- Return to sports sooner
There were some significant limitations to this study. They could not blind researchers to parts of the ASKp tool, there was high loss to follow-up and no intention to treat analysis. The authors conclusions were ” Children treated with removable splinting have a better physical functioning and less difficulty with activities than those treated with a cast.”
Now let us jump ahead to some more recent literature. These two studies look at greenstick fractures and/or transverse fractures of the distal radius that are minimally displaced. Buckle fractures were specifically excluded from these two studies. Therefore, these studies represent more serious fractures and risk of complications.
Reference: Kropman et al . Threatment of impacted greenstick forearm fractures in children using bandage or cast therapy a prospective randomized trial. J Trauma 2010
- Population: Children 4-13y presenting to ED with impacted greenstick fractures of the distal 1/3 of radius or ulna
- Intervention: Soft bandage wrapping treatment (BT) for 4 weeks
- Control: Below elbow backslab cast for 1 week followed by circumferential cast treatment (CT) for 3 weeks
- Outcome: 1) Pain, 2) Discomfort, 3) Function, 4) Fracture displacement
Results:
- Pain: more in first week only of BT group
- Discomfort: no difference in use of pain killers and less itching in BT group
- Function: quicker return to normal function with BT
- Fracture Displacemet: No difference in secondary angulation and no refractures in either group
Authors’ Conclusions: “BT for impacted greenstick fractures of the distal forearm is a safe technique, patients treated with bandage suffer greater pain at the start of the treatment, are able to return to normal activities sooner, and have less discomfort when compared with the standard CT.”
BEEM Commentary: This is a well-conducted randomized trial. The patients are genearlizable to the population presenting to the ED and the oucome measures are clinically relevant. The sample size is moderate (n=90)
BEEM Bottom Line: As long as parents are aware that BT is associated with increased pain in the first week post-injury, this is a safe alternative to traditional casting. Patients will be more likely to return to normal function faster and experience less itching.
Reference: Boutis et al. Cast vs. Splint in Children with Minimally Angulated Fractures of the Distal Radius: A Randomized Control Trial. CMAJ 2010
- Population: Convenient sample of children age 5-12 yrs presenting to ED with minimally angulated/displaced greenstick or transverse fractures of the distal radius (EXLUDED buckle/growth plate or open fractures)
- Intervention: Prefabricated wrist splint worn for 4 weeks
- Control: Short arm fibreglass cast worn for 4 weeks
- Outcome: Primary: physical function at 6 weeks using (ASK), Secondary: fracture angulation, pain, use of splint, grip strength, patient preference
Results:
- Primary: No difference in ASK score at 6 weeks mean 1.44 (95% CI -1.75 to 4.62)
- Secondary: No difference in fracture angulation, pain, grip strength BUT patient and parental preference was for a splint
Authors’ Conclusions: “In children with minimally angulated greenstick or transverse fractures of the distal radius, use of a prefabricated splint was as effective as a short arm cast with respect to recovery of physical function. In addition, the devices did not differ significantly with regard to the maintenance of fracture stability and the occurrence of complications, and the splint was superior to the cast in terms of parental and patient satisfaction and preferences.”
BEEM Commentary: This is a well conducted randomized trial of 96 children. The methodology was sound and the follow-up was excellent. The researchers focused on clinically-relevant outcomes and there was no significant differences found between the cast group and the splint group. This is the first study examining this research question and further studies will help solidify these conclusions.
BEEM Bottom Line: Splinting appears to be a viable option for minimally angulated/displaced fractures of the distal forearm in children.
Further Reading:
- Ransborg and Siversten. Distal radius fractues in children: substantial difference in stability between buckle and greenstick fractures. Acta Orthopaedica 2009. They concluded that buckle fractures are stable, do not requrie follow-up and 6/207 had mild complication because of plaster casting.
- Abraham et al. Interventions for treating wrist fractures in children. Cochrane 2008
 Case Scenario Conclusion: A discussion was held with the father about his nine-year-old ringette star. Risks and benefits of casting vs. splinting/BT was reviewed. A shared decision was made to remove the cast and go with a splint. He also preferred following up with his local primary care physician in two weeks rather than driving one hour to the pediatric orthopedic fracture clinic. The patient did well and is back on her team with full function.
Case Scenario Conclusion: A discussion was held with the father about his nine-year-old ringette star. Risks and benefits of casting vs. splinting/BT was reviewed. A shared decision was made to remove the cast and go with a splint. He also preferred following up with his local primary care physician in two weeks rather than driving one hour to the pediatric orthopedic fracture clinic. The patient did well and is back on her team with full function.
KEENER KONTEST: Last weeks winner was Daniel Beamish who is studying medicine in Australia. He correctly identified GMEP as the Global Medical Education Project. Defined by its founder Dr. Mike Codogan as the “The Facebook of medicine. A place to share medical videos, discussion, questions and conversation without feeling über nerdy.” If you have not joined this FOAMed movement then what are you waiting for?
Listen to the podcast to hear this weeks Keener Kontest question.
Email your answer to TheSGEM@gmail.com. Use “Keener Kontest” in the subject line. First person to email me the correct answer will win a cool skeptical prize.
OK all you procrastinators, time is running out to sign up for take advantage of SkiBEEM 2013 Feb 4-6 at SilverStar BC. You want the most current EBM reviews from 2012 then email Teresa. Cut your KT window to less than one year. We are even planning on even doing a live episode of TheSGEM as a PUBcast at the conference!
![]()
Remember to be skeptical of anything you learn, even if you heard it on The Skeptics’ Guide to Emergency Medicine.




{kind=link}
{kind=link}
You must be logged in to post a comment.